응급실에서 발급된 소아 사망진단서 오류
Errors in pediatric death certificates issued in an emergency department
Article information

Trans Abstract
Purpose
Errors in pediatric death certificates (DCs) have been rarely reported. We analyzed the errors in writing the DCs issued in an emergency department (ED).
Methods
The DCs issued at the ED to patients aged 18 years or younger were retrospectively analyzed. Their medical records were reviewed by 4 emergency physicians. Major and minor errors in the DCs were defined based on the International Statistical Classification of Diseases and Related Health Problems 10th revision guidelines. The DCs were classified into the disease group and the external group by the manner of death, and the errors were compared.
Results
Among a total of 87 DCs issued in the ED, 97.5% and 100% were confirmed to contain at least 1 error in the disease (n = 40) and external (n = 47) groups, respectively. The median numbers of errors in the analyzed DCs were 2.0 and 3.0 in the disease and external groups, respectively (P = 0.004). In the disease group, the most frequent major error was reporting only a secondary condition as the underlying cause of death without antecedent causes (6 cases [15.0%]). In the external group, the most frequent major error was writing 2 or more causes in a single line for the cause of death (17 cases [36.2%]). In both groups, the most common minor error was omission of a time interval record for the cause of death (disease, 37 cases [92.5%]; external, 42 cases [89.4%]).
Conclusion
Any errors were identified in 98.9% of pediatric DCs issued in the ED, and the total number of errors was larger in the external group.
Introduction
Death certificates (DCs) have been reported to contain multiple errors1-12). The errors reduce the certificate’s value as a medical document, and adversely affect the quality of studies and statistics related to the causes of death (CODs). Such errors can be reduced by simple training in writing DC and various types of intervention1-4,6-10). Most studies on defective DCs targeted adults1-4,7,8,11,12), and did not consider the characteristics of pediatric DCs. To the authors’ knowledge, only 1 study reviewed errors in pediatric DCs5) without review of medical records, thereby reducing the accuracy in determining the COD and in the analysis of errors in DCs. In addition, the study did not analyze various errors comprehensively. Pediatric DCs are valuable resources for health care policy and child mortality statistics, suggesting the need for further investigation. Thus, we aimed to analyze errors in pediatric DCs issued in an emergency department (ED).
Methods
1. Study design and setting
This study was a retrospective analysis of DCs involving patients aged 18 years or younger issued at the ED of the Ulsan University Hospital located on the southeastern coast of Korea from 2005 to 2020. The study was approved by the institutional review board with a waiver for informed consents (IRB no. UUH-IRB-2021-06-072). Errors in the DCs were investigated based on the World Health Organization International Statistical Classification of Diseases and Related Health Problems 10th Revision guidelines13). The errors were evaluated based on medical records of the deceased. The records were primarily reviewed by 3 emergency physicians currently working in the ED who are experienced in writing DCs. A senior emergency physician with 20 years of clinical experience at the ED performed the second review. In the case of disagreement after the second review, a final consensus was reached by the 4 physicians. DCs issued with an unknown COD even after the final consensus were excluded from the study.
2. Definitions of the errors and variables of interest
Errors were divided into major and minor according to the previously described criteria2,3,5,10-12,14-18). The errors are listed in Table 1 and Appendices 1, 2 (https://doi.org/10.22470/pemj.2022.00444). Variables of interest included sex, age (years), age groups (0-1, 2-6, 7-12, and 13-18 years), number of lines filled up for CODs, number of CODs recorded in the DCs, numbers of the errors (total, major, and minor), and detailed number of each subcategory of the errors. According to the manner of death, including disease and external causes, the cases were classified into the disease and external groups for comparison of such errors between the groups. Subsequently, the errors were compared between the groups using chi-square tests, Fisher’s exact tests, and Mann-Whitney U-tests. IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY) was used for the statistical analysis. Statistical significance was defined as P < 0.05.

Definitions of the major errors in death certificates
Results
Among the 2,309 DCs issued from 2005 to 2020 at the ED, 100 were for patients aged 18 years or younger. Thirteen DCs with unknown CODs were excluded from the study. The 87 remaining cases of DCs were divided into the disease group (40 cases [46.0%]) and the external group (47 cases [54.0%]). The most common COD in children aged 1 year or younger was disease (21 of the 26 children). The most common COD in those aged 13-18 years was external causes (25 of the 35 children). Among the 4 lines provided for COD in the form, the median numbers of filled lines were 2.0 in both groups. The most common number recorded CODs was 1 and 2 in the disease (40.0%) and external (34.0%) groups, respectively. The disease group revealed 97.5% of errors, and the external group 100%. The median numbers of the total and minor errors were larger in the disease group than in the external group without a difference in the median numbers of the major errors (Table 2).

Characteristics of DCs according to the manner of death
In the disease group, the most frequent major error was reporting only a secondary condition as the underlying COD without antecedent causes (6 cases [15.0%]). In the external group, the most frequent major error was writing 2 or more causes in a single line for COD (17 cases [36.2%]). The mode of death was recorded as an underlying COD in 4 cases (10.0%) in the disease group and 2 cases (4.3%) in the external group (Table 3).
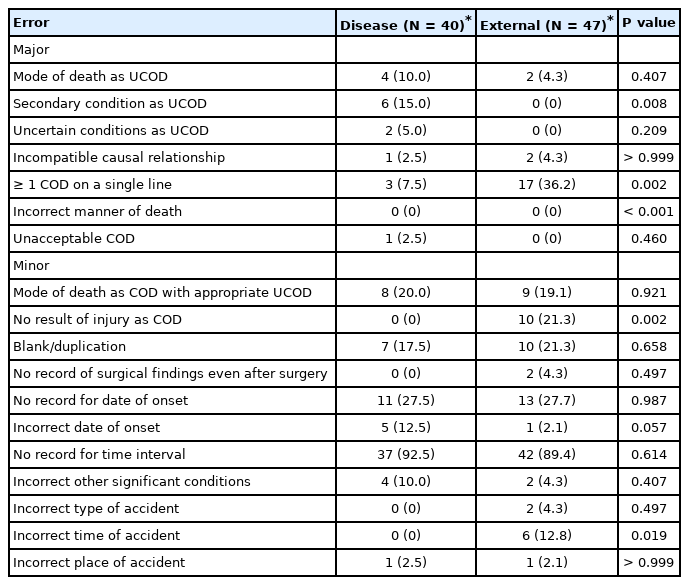
Major and minor errors in pediatric death certificates according to the manner of death
The most common minor error was omission of a time interval record for COD in both groups (disease, 37 cases [92.5%]; external, 42 cases [89.4%]) (Table 3). Omission of the date of onset was found in 11 cases (27.5%) and 13 cases (27.7%) in the disease and external groups, respectively. The mode of death as the direct COD was recorded despite an appropriate underlying COD in 8 cases (20.0%) and 9 cases (19.1%) in the disease and external groups, respectively. Ten cases (21.3%) in the external group did not include accident-related information as the underlying COD although the type of accident was recorded (see “No result of injury as COD” in Table 3).
Discussion
This study analyzed various types and frequencies of errors in pediatric DCs by reviewing the medical records. One or more errors were found in 86 of the 87 DCs (Table 2). Previous studies confirmed multiple errors involving DCs1-12). Likewise, several errors were found in this study. The finding of writing 2 or more CODs in single line as the most common major error in the external group suggests that the principles of writing DC were not fully understood by emergency physicians4,8). It was difficult to retrospectively determine which the direct COD was when more than 1 was written in a single line.
The most common minor error was the omission of a time interval record in both groups, followed by omission of the date of onset. This type of errors is commonly found in adult DCs2,3,5,10,11). Emergency physicians usually record the date of death, rather than that of onset, on pediatric DCs. This behavior is probably due to the difficulty in obtaining the date of onset while caring for critically ill or injured children8). Although the time interval is not a critical item in DCs, it is important to fill in the details to determine the temporal sequence leading to death and to infer a causation.
A recent study analyzing errors in DCs related to external causes reported that the number of errors increased with the number of descriptions of COD11). In the present study, total errors tended to occur more frequently in the external group, which had more lines filled up for COD (P = 0.043).
Among the 21 infant cases in the disease group, 8 had sudden infant death syndrome (SIDS) as CODs. This finding suggests the relevance of SIDS in DCs19). In cases of SIDS, COD cannot be explained even after thorough history taking and investigation at the time of death, and autopsy. Although SIDS indicates an unknown COD, it is still acceptable as a COD.
Asphyxia is a more apparent COD than SIDS. Both conditions can be determined as a COD after ruling out other possible candidates. Thus, it is essential to comprehensively determine the COD after a detailed history taking, physical examination, and all possible objective investigations before writing a DC. CODs written in EDs are often subject to changes after additional investigation, such as autopsy. However, the potential change in the CODs remains acceptable if they were written based on the emergency physician's expertise and objective findings at the time of writing the DC.
If the COD is recorded as unknown, it is classified as a possible COD during the final compilation of the national statistics on CODs, which may contribute to erroneous statistics. When emergency physicians write DCs, it is necessary to minimize description of an unknown COD to prevent inaccuracies, based on direct review of medical information related to the COD. Errors can be reduced through simple training and education9).
In the cases of children aged 13 to 18 years, more cases were classified into the external group. The errors in DCs were more frequently found in the external group than in the disease group. Information regarding the external causes, such as the location, time, type, and intention of the accident, may be prone to errors.
In the case of death due to an external cause, children often died before arrival at EDs. The mechanism of death is important for the statistics on CODs while the partial contribution of injury to death is less relevant. Thus, the mechanism should be written accurately even in a case of death due to multiple injuries prior to sufficient investigation. The injury that has the most decisive effect at the time of death should be selected as the direct COD. The other injuries should be described in the “other significant conditions” in DCs. The injuries should not be written on the same line.
This study included only pediatric DCs issued in the ED, implying the difficulty in generalizing the findings. However, it may serve as a groundwork for additional studies on errors in pediatric DCs. Another limitation is that we could not investigate potential factors affecting the writing of DCs, such as the level of training and clinical experience in the ED. Finally, 5 infant cases were excluded since they had unknown CODs in their DCs. This exclusion might be related to underestimation of impact of SIDS on DCs because the 5 cases could also be considered as SIDS.
In conclusion, 1 or more errors were identified in 98.9% of pediatric DCs issued in the ED. Errors were more common in the external group than in the disease group. In the disease and external groups, the most frequent major errors were reporting only a secondary condition as the underlying COD without antecedent causes and writing 2 or more causes in a single line for COD, respectively. The most common minor error was omission of a time interval record for the COD in both groups. Errors in writing DCs can be minimized by continuous education and feedback for emergency physicians.
Notes
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Funding sources
No funding source relevant to this article was reported.
Acknowledgements
The authors are grateful to Dr. Soobeom Park and Dr. Sangyeop Jung (Department of Emergency Medicine, Ulsan University Hospital, University of Ulsan College of Medicine) for their contribution in collecting data.
References
Appendices

Examples of common errors (a) and corrections for the errors (b) in death certificates in cases of disease (A) and of external cause (B). Major errors are marked with (★) and minor errors are marked with (■). A 4-year-old boy with underlying diabetes mellitus visited the emergency department with fever and cough for 3 days. Progressive mental change, dyspnea, and hypotension occurred in 1 hour after the visit. He died in 6 hours after the visit. The initial chest radiograph showed severe pneumonic consolidation (A). After a pedestrian accident, a 7-year-old boy obtained injuries in the head, chest, and pelvic bone. He was transported to the emergency department with a state of cardiac arrest. He died after 30 minutes of cardiopulmonary resuscitation (B).
