







Introduction
Esophageal perforation (also known as Boerhaave syndrome) is uncommon but fatal. Particularly in children, it is challenging to diagnose and treat the disease entity. The esophagus is an anatomically inaccessible organ that is close to important structures, such as the great vessels and trachea. The perforation is usually caused by prolonged or forceful vomiting and retching, ingestion of bones or iatrogenic causes, such as surgery, endoscopy or biopsy. We report an adolescent girl who developed esophageal perforation after consuming a large number of caffeine tablets for suicide attempt. This study was approved by the institutional review board of Hanyang University College of Medicine (IRB no. 2022-09-013).
Case
A previously healthy 13-year-old girl visited the emergency department with a 2-hour history of repetitive vomiting and chest pain. Her symptoms were not improved with antiemetic therapy. She had eaten meals mainly consisting of snacks because of decreased appetite and continuous nausea from 9 months before. She was living with her divorced father and an older sister.
The initial vital signs were as follows: blood pressure, 110/60 mmHg (67th and 41st percentiles, respectively); heart rate, 110 beats/minute; respiratory rate, 20 breaths/minute; temperature, 37.6°C; and oxygen saturation, 97% on room air. At that time, the girl did not report any symptoms, such as dyspnea. On physical examination, she was alert and did not show signs of respiratory distress, such as chest retraction or decreased breathing sound.
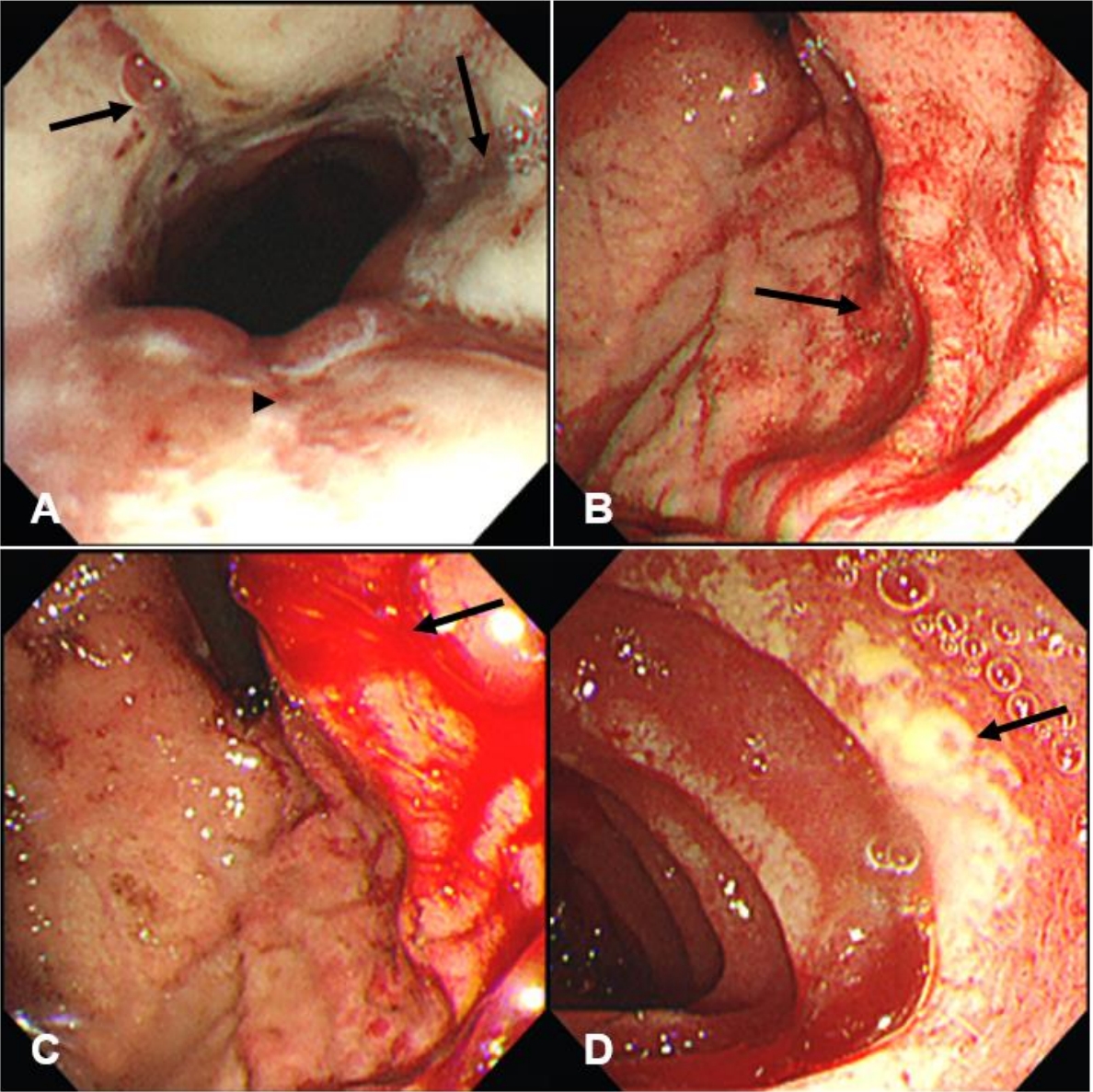
The initial chest radiograph showed subcutaneous emphysema and pneumomediastinum (Fig. 1). Computed tomography of the chest showed the findings of esophageal perforation (Fig. 2). On day 2, upper gastrointestinal (UGI) endoscopy showed deep longitudinal tears and ulcers with hemorrhage in the distal esophagus (Fig. 3). The endoscopy also showed the ulcers, edematous wall thickening, and blurring of tissue interface on the whole UGI mucosa, particularly severe in the esophagus. Laboratory findings showed a leukocyte count of 26,800/mm³ with 87% neutrophils and C-reactive protein concentration of 1.4 mg/dL.
During hospitalization, the girl disclosed that she had taken 50 tablets of caffeine supplements (270 mg/kg) in a suicide attempt before the onset of vomiting. After she was severely bullied at an elementary school, she suffered from anxiety and fear that she would be bullied again even if she made some friends. In addition, she first revealed another suicide attempt by ingesting a large amount of caffeine, which occurred 1 year before this visit. For the esophageal perforation, we performed conservative therapy, such as oxygenation and analgesia, by virtue of relatively stable vital signs, a continuous decrease in need for oxygen, and the absence of signs of sepsis. She was also kept nil per os, and administered intravenous ceftriaxone (50 mg/kg/day) and metronidazole (40 mg/kg/day), antiemetics, and a proton pump inhibitor.
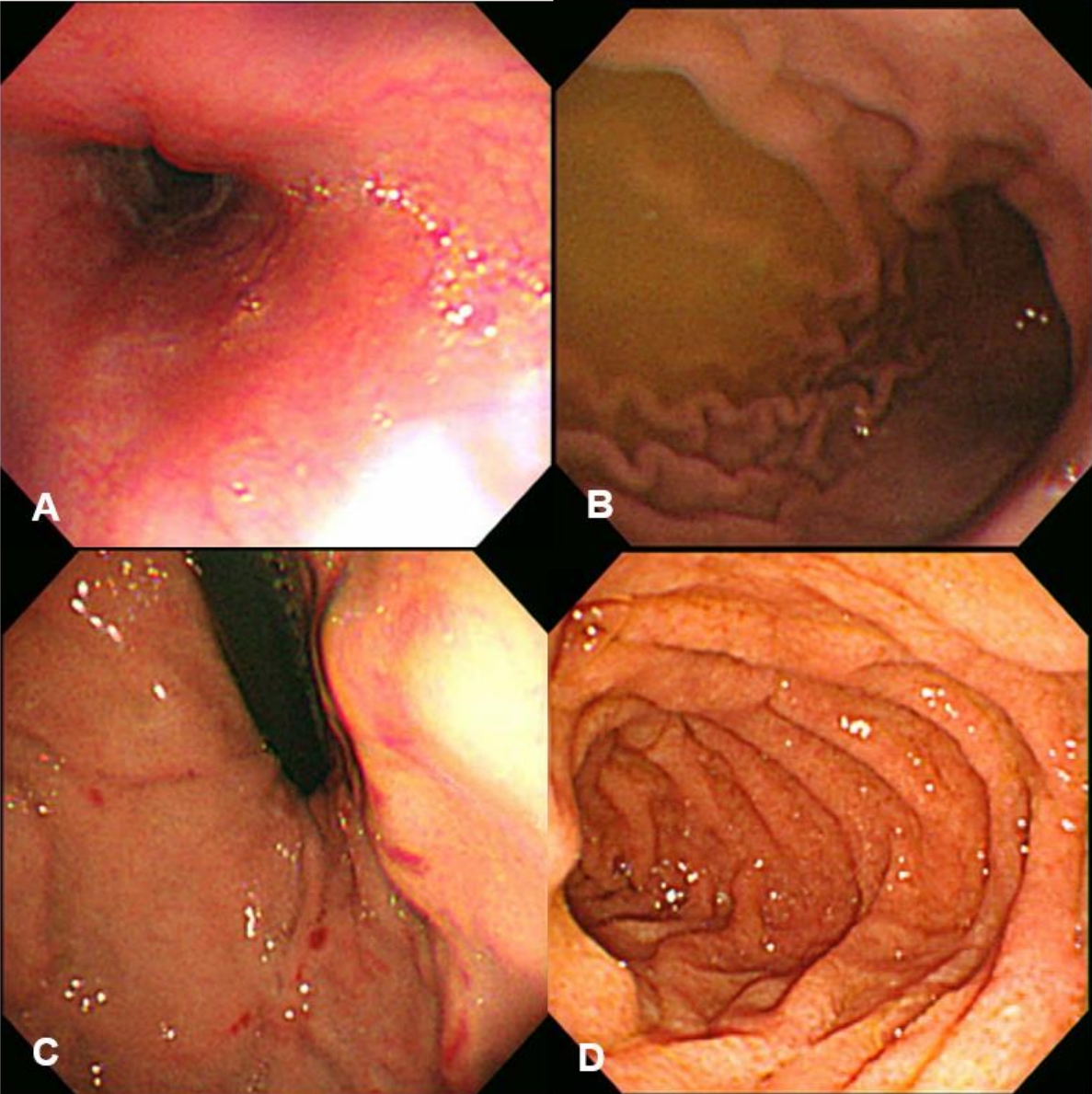
A follow-up computed tomography on day 3 showed improving findings of the emphysema and pneumomediastinum. A follow-up endoscopy performed on day 13 also showed an improved state of the ulcers on the whole UGI mucosa and a good patency of the esophageal lumen, but the bleeding continued in the distal esophagus (Fig. 4). Afterwards, oral nutrition became possible, and she was discharged uneventfully on day 20.
Discussion
Esophageal perforation needs early diagnosis and treatment given its high mortality and morbidity1). This case was caused by the suicidal ingestion of caffeine tablets. The ingestion resulted in the perforation, primarily via caffeine-induced forceful vomiting, and secondarily via caffeine-induced gastric acid secretion and smooth muscle relaxation, and via the large number of tablets-induced sudden increase in intra-esophageal pressure. Although it is rarely associated with esophageal perforation, suicide attempt should be considered at the initial presentation given that it is the leading cause of death in adolescents.
Esophageal perforation is still difficult to treat although its mortality rate is gradually decreasing due to the development of diagnostic technology and new antibiotics. Because the esophagus does not have the serosa, the perforation leads to mediastinitis, empyema, sepsis, and eventually death. In addition, the risk of drug-induced esophageal injury is highly found in the anatomic constrictions at the aortic arch, left main stem bronchus, and gastroesophageal junction2). It is probable when ingested pills are in contact with the esophageal mucosa for a long time. Pill size and formation can also affect it2,3). Large pills are more commonly retained in the esophagus than smaller pills2). In addition, it may be more damaging in the case of ingesting sustained release formations or gelatin capsules, which are able to adhere to the mucosa3).
Caffeine is one of the most widely used drugs and a well-known stimulant that belongs to the plant alkaloid family. The substance is contained in some commonly consumed powder, tablets, food or beverage, such as coke and chocolate4). This ubiquity indicates that the amount of caffeine consumed, even in unintentional ingestion, may be much larger than felt by the consumers. Caffeine relaxes the smooth muscles and blood vessels of the digestive system, and promotes secretion of the gastric acid. When caffeine is consumed excessively, the gastric mucosa is damaged due to the excess gastric acid, and heartburn can be aggravated by gastroesophageal reflux. Caffeine poisoning can cause vomiting, damage to the mucous membrane, and hypokalemia5).
At a dose of 150-200 mg/kg or more, caffeine can cause arrhythmia, seizure, rhabdomyolysis, acute kidney injury, and other fatal outcomes. Acute ingestion manifests as vomiting, electrolyte abnormalities, convulsions, headaches, and arrhythmia. Also, patients who take caffeine chronically may experience erosive esophagitis, gastric ulcer, tachycardia, headache, palpitations, insomnia or delirium. Currently, single-ingredient caffeine oral formulations are not officially produced in Korea. However, there may be cases where the tablets produced in foreign countries are purchased for temporary arousal or weight control, and there are currently no special regulations or warnings for this. The case patient had repeatedly consumed a large amount of caffeine for the suicide attempts for 1 year. At the visit, the ingested dose was 270 mg/kg (10,000 mg). Despite the lethal dose, she did not show fatal toxidrome other than the esophageal perforation due to recurrent vomiting. We speculate that the actually absorbed amount was insufficient to cause cardiac or neurologic manifestations owing to the decreased absorption by severe vomiting and perforation.
Therapeutic modality for esophageal perforation should be decided by considering the cause of perforation, underlying esophageal diseases, and lapse of time from perforation to diagnosis. Therapeutic goals are to prevent the mediastinal contamination, mitigate inflammation, ensure the esophageal continuity, and restore and maintain nutrition. Surgical principle is to remove the infected or necrotic tissue, finely suture the site of perforation, and drain the contaminated and infected area. However, when the perforation is confined to the mediastinum without a leak to the surrounding tissue and lacks signs of sepsis, conservative therapy is indicated as in the case patient. The conservative therapy encompasses keeping nil per os, adequate parenteral nutrition, broad-spectrum antibiotic therapy, and if needed, drainage through chest or nasogastric tubes.
The authors report a case of esophageal perforation caused by suicidal caffeine poisoning in an adolescent girl. Experiencing this patient, we would like to remind that it is vital to consider poisoning when teenagers with unusual symptoms visit emergency departments.