A case of successful removal of a zipper entrapped on the upper eyelid of a child using a lidocaine gel
Article information
Abstract
Zipper entrapment injuries require a technique to safely and promptly release the entrapped tissues to prevent complications. Herein, we report an 8-year-old girl whose eyelid was successfully released from an entrapping zipper. She presented to the pediatric emergency department with her right upper eyelid entrapped in a zipper while getting dressed. She was distressed, anxious, and crying in pain. We have successfully removed the zipper using a lubricating gel, which provides local anesthesia. This case report will increase emergency physicians’ awareness of the technique of removing an entrapped zipper on the eyelid using a lidocaine gel.
Introduction
Zipper entrapment injuries are common but can cause physicians to fluster if they are unfamiliar with the appropriate management strategies in emergency departments (EDs). In a case series conducted on patients aged 2-12 years in an ED, the incidence of zipper entrapment injury was approximately 1 in 4,000 patients. Most injuries were easily managed in EDs without general anesthesia and involve entrapment of the penis or scrotal skin in the zipper teeth while being pulled up (1-4). We found only 2 pediatric cases of eyelid zipper injury (5,6). In one case, the zipper was removed after cutting along the side of the zipper teeth to relieve tension on the entire zipper system with intranasal fentanyl used for analgesia (5). In the other case, lidocaine with epinephrine was used as an anesthetic with constrictor, and the zipper was gently released (6).
To minimize direct tissue damage, pain, scarring, and complications, the skin entrapped in the zipper should be gently released. Here, we report a girl with her eyelid entrapped in a zipper who was successfully treated in the ED. This study adhered to the ethical standards outlined in the Declaration of Helsinki. Due to the retrospective nature of the study and the fact that the patient’s identity is not directly exposed, the institutional review board of Severance Hospital has waived the need for informed consent (IRB no. 4-2023-1660).
Case
An 8-year-old girl presented to the pediatric ED with her right upper eyelid entrapped in a zipper. In detail, while putting her head in a jacket, she tried to pull the zipper up, and the eyelid became entrapped. Although she herself, her parents, and even a called emergency medical technician tried to unzip it, it only caused pain, leaving the entrapment unreleased. Consequently, she was brought to the ED with the upper half of her face covered by the rest of the jacket cut off, only leaving approximately 15 cm above the entrapping zipper (Fig. 1). At the arrival, she was distressed, anxious, and crying with her pain. She had no bleeding disorders or other previous medical conditions, and was up to date for the scheduled tetanus immunization.

An 8-year-old girl with the right upper eyelid entrapped in a zipper.
An approximately 1-cm segment of the right upper eyelid was entrapped in the lower back portion of the zipper teeth (Fig. 2A). She reported fear and pain when blinking or moving the jacket with the attached zipper. There was no impairment of extraocular movements, the pupils were equal and normally reactive, and the conjunctiva was clear, without any visible active bleeding or trauma elsewhere.
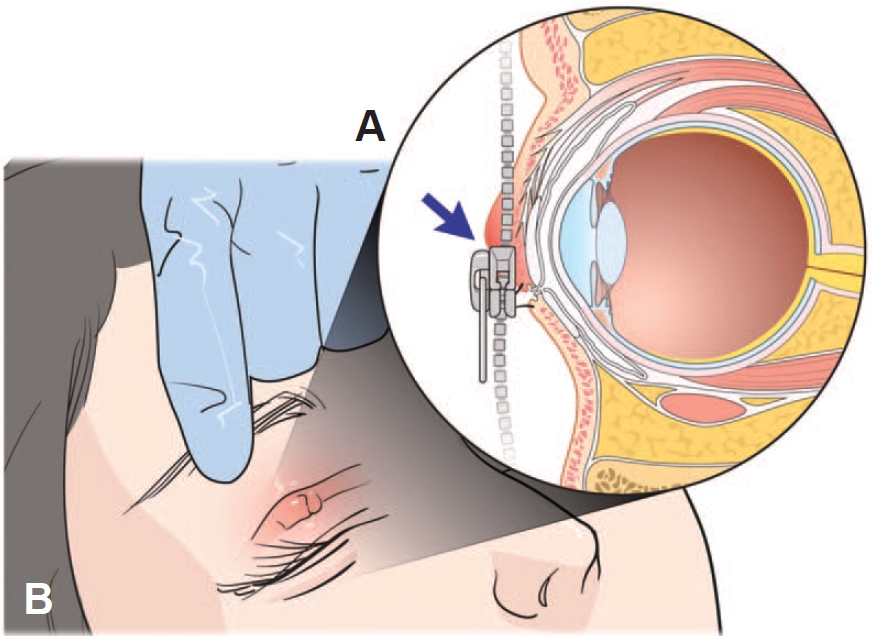
The right upper eyelid entrapped in the lower back portion of the zipper teeth (arrow, A). After releasing the eyelid, there remains an approximately 0.7-cm linear pinched skin with mild erythema (B).
For analgesia and lubrication prior to releasing the zipper, a commercially available lubricant (InstillagelTM, Farco-Pharma GmbH) was applied to the skin surrounding the engaged eyelid. The lubricant is a sterile gel containing lidocaine and chlorhexidine provided in a syringe-like sterile package, and is usually used for urological procedures, such as urinary catheter insertion. Sterile gauze and paper tape were used to cover the right eyebrow and globe to prevent the gel from irritating the cornea or conjunctiva, with the entrapped eyelid exposed only before application. During the procedure, a trained pediatric nurse and the girl’s father provided distractions, such as deep breathing, holding her hands, counting to 100, and questions about what she wanted to do after the treatment was over, in order to reduce her fear and keep her comfortable. After 5 minutes, once lidocaine had taken effect and reduced the pain, the slider piece of the zipper was slowly released manually from the eyelid skin by the emergency physician.
After complete removal of the zipper, the girl had a 0.7-cm linear pinched skin with mild erythema on the eyelid, without a laceration and bleeding (Fig. 2B). Her extraocular movements remained intact, and there was no decrease in visual acuity or visual field defect. She was discharged with an antibiotic ointment prescribed. Her father did not want a follow-up appointment at the ophthalmology clinic because of the distance from home.
Discussion
In this current case, we provided both analgesic and lubricating effects using the abovementioned lubricant in a syringe form. Without the need to administer drugs through alternative routes for anesthesia, we were able to reduce pain in local areas while concurrently providing a lubricating effect, thus streamlining the overall procedure.
Various techniques for zipper release have been described in the literature, such as cutting, pulling, and twisting. The most commonly used technique is cutting the median bar of the zipper. For this purpose, a robust wire or surgical bone cutter is occasionally used, or a small hacksaw in some cases (3,4,7). Cutting the median bar separates both sides of the zipper teeth from each other, releasing the entrapped skin (7-9). However, this technique may require special tools since the median bar may not be easily accessible depending on the angle and type of the zipper (10). Another commonly used one is gently pulling the lubricated zipper on to release the entrapped skin (10,11). Other techniques include twisting a small flathead screwdriver between the 2 faceplates of the zipper to widen the gap or using trauma scissors or a needle holder to remove the teeth; however, these have the risk of damaging the entrapped skin (2,8,11). In other literature that compared different techniques of removing zippers from the entrapped skin, lubrication with mineral oil was most preferred and successful among both novice and experienced providers (11).
The use of local anesthetics, per os or intravenous analgesics, or procedural sedation depends on the patient’s age and level of cooperation. This may help make the patients comfortable and cooperative (7,8,10). In this current case, the girl was 8 years old, and the zipper was removed without procedural sedation and analgesia. Instead, only local anesthesia with the lidocaine-containing lubricant was used, along with distraction methods, which are described in the case section. If attempts to remove the zipper at the bedside using the various methods above are unsuccessful, consultation with an appropriate specialist is required to remove it in the operating room under general anesthesia (8,10).
The optimal releasing technique should be swift not to further injure the already damaged tissue, which may become infected. After the zipper is released, it is crucial to take precautions at home to prevent infection of the affected skin. Guardians should be educated on the application of antibiotic ointment or cream against any superficial laceration or abrasion.
In conclusion, children’s zipper entrapment injuries can be encountered in EDs. To ensure a safe and prompt release of the entrapped skin and prevent complications such as tissue damage and scarring, knowledge about various releasing techniques and post-procedural management may be helpful to the relevant emergency practices. The knowledge can be provided by this care report, which describes a rare case of zipper injuries entrapping the eyelid and discusses the various releasing techniques.
Notes
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
Funding sources
No funding source relevant to this article was reported.
Author contributions
Conceptualization and Investigation: all authors Resources, Supervision, and Project administration: S Hwang
Visualization: SY Choi
Writing-original draft: SY Choi
Writing-review and editing: all authors
All authors read and approved the final manuscript.
Data availability
All data presented in this manuscript are available from the corresponding author upon reasonable request.
Acknowledgements
We extend our sincere thanks to the patient and her father for their cooperation in this study, and MID (Medical Illustration & Design), as a member of the Medical Research Support Services of Yonsei University College of Medicine, providing excellent support with medical illustration.