소아응급실을 통해 입원한 소아환자의 특성과 소아응급병동의 입원 효과
Abstract
Purpose
To evaluate the efficiency of the pediatric emergency ward (PEW) through the outcomes of children hospitalized to the ward by the department of pediatric emergency medicine (PEM).
Methods
A chart review was completed for children (< 15 years) who were hospitalized to the PEW via the pediatric emergency center from March through May 2021. We compared the general characteristics and details regarding the outcomes depending on the departments they were hospitalized to, namely PEM, pediatrics (PED), and others.
Results
We analyzed a total of 606 hospitalized children: PEM, 91; PED, 456; and others, 59. In the order listed above, their median ages were 2 years (interquartile range, 1-6), 1 year (0-4), and 9 years (7-14) (P < 0.001). The numbers of children with Korean Triage and Acuity Scale of 1-3 were 71 (78.0%), 400 (87.7%), and 33 (55.9%) (P < 0.001). Median length of stay (LOS) in the emergency department (ED) and hospital tended to be shorter in PEM (ED LOS: PEM, 4.3 hours vs. PED and others, 4.0-6.3 hours; hospital LOS: PEM, 19.0 hours vs. PED and others, 58.5-63.8 hours; all Ps < 0.001). The differences in the LOS were prominent between others and PEM (ED LOS, 1.538 [95% confidence interval, 1.353-1.749]; hospital LOS, 3.375 [2.741-4.157]). Transfers to other departments occurred only in PEM (4.4%) and PED (3.9%) whereas intensive care was performed only in others (27.1%). Return visits showed no difference among the 3 departments. Top 5 chief complaints and primary diagnoses of the children hospitalized to PEM were vomiting, fever, abdominal pain, head injury, and poisoning, and gastroenteritis, concussion, syncope, poisoning, and upper respiratory infection, respectively.
Conclusion
Hospitalization to PEWs for short-term treatment or observation may relieve overcrowding in EDs or in hospitals, with comparable frequency of return visits.
Key Words: Efficiency; Epidemiology; Hospitalization; Length of Stay; Pediatric Emergency Medicine
서 론
출산율 저하 및 소아인구 감소에도 불구하고 소아환자(환자)의 응급실 방문은 늘어났다( 1, 2). 또한, 코로나바이러스병-19를 비롯한 신종 감염병이 등장하고 사회 활동 및 맞벌이 부부가 늘면서 소아∙청소년이 밤, 주말, 공휴일에 의료기관을 방문하는 경우가 늘고 있다( 3, 4). 국가응급환자진료정보망 자료에 따르면, 2022년 12월 현재 한국에서 24시간 전문의 진료가 가능한 소아전문응급의료센터(소아응급센터)가 8개소이고, 이곳을 중심으로 응급진료가 이뤄지고 있다( 5). 다만, 최근 소아 인구 감소 및 소아응급의료 인력 확보의 어려움으로 인해 24시간 진료에 제한이 있다( 6). 이에 따라 환자가 24시간 응급진료가 가능한 소수 병원으로 몰리고 그 병원의 병실이 제한되어, 응급실이 과밀화되고 있다( 7). 응급실 체류가 길어질수록 환자 예후 및 만족도는 나빠진다( 8, 9). 또한, 환자 중 비교적 중증인 한국형 응급환자 분류도구(Korean Triage and Acuity Scale, KTAS) 1-2단계는 5.9%에 불과하다( 10). 이중 일부는 응급실에 재방문 하는데( 11, 12), 이 또한 응급진료의 효율성을 떨어뜨리고 진료의 질적 악화로 이어진다( 13, 14). 이 문제를 해결하기 위해 소아응급센터에서 단기 입원 해야 하는 환자를 대상으로 응급병동을 운영했고, 이에 따른 응급실 체류시간 및 재방문이 감소하고 응급병동 입원을 다른 진료과 입원과 비교하여 예후에 차이가 없을 것으로 기대했다. 본 연구는 단일기관 소아응급센터를 통해 소아응급의학과, 소아청소년과(소아과), 기타 진료과에 입원하는 소아∙청소년 환자의 일반적 특성을 확인하고 이를 분석함으로써, 소아응급센터가 운영하는 응급병동의 유용성을 확인하고 추후 운영 방향을 모색하고자 했다.
대상과 방법
분당차병원 소아응급센터는 연평균 25,000명의 18세 이하 환자가 방문하고, 2021년 현재 한국의 8개 소아응급센터 중 한 곳이다. 본 저자가 알기로는 한국에서 소아응급의학과로 단기 입원하는 병원은 본원이 처음이며, 관련 연구가 부족한 실정이다. 본 연구는 본원 응급병동 시범 운영 기간인 2021년 3월 1일-5월 31일에 상기 센터를 경유하여 병동에 입원한 15세 미만 환자를 대상으로 했다. 후향적 연구로, 본원 임상연구심사위원회의 승인을 받았고, 의무기록을 이용한 통계적 연구로 연구대상자 동의는 면제됐다(IRB no. CHAMC 2023-02-064).
연구기간에 센터 방문 후 입원한 환자를 입원 진료과에 따라 소아응급의학과, 소아과, 기타 진료과로 나눴다. 응급실 방문 당시 수집한 변수는 KTAS(응급: 1-3단계), 성별, 나이, 발병 후 방문까지 소요 시간(분), 구급차 탑승, 의식상태, 활력징후(혈압, 심박수, 호흡수, 체온, 산소포화도), 응급실 체류시간(시간), 입원 기간(시간), 입원 진료과, 주요호소증상(주증상), 주진단을 수집하여 비교 분석했고, 입원 후 결과(전과[轉科]) 및 중환자실 입원) 및 재방문(7일 이내 같은 증상) 여부를 확인했다.
통계적 분석에 R version 4.2.1(R foundation for Statistical Computing)을 사용했다. 연속형 변수는 중앙값 및 사분위수 범위로, 범주형 변수는 수 및 백분율로 각각 표시했다. 세 군을 비교할 때, 연속형 변수는 Kruskal-Wallis test, 범주형 변수는 Pearson’s chi-square test 또는 상기 프로그램의“fisher.test”를 이용한 exact test를 시행했다. 선형 연관을 추정 및 검정하기 위해 단일 독립 변수에 대해 단순 선형회귀분석을 시행했다. 구체적으로, 독립변수인 진료과에 대한 단변수 분석으로, 종속변수를 응급실 체류시간 및 입원 기간으로 구분하여 회귀분석을 시행했다. P가 0.05 미만인 경우 통계적 유의성을 갖는 것으로 정의했다.
결 과
1. 일반적 특성
연구기간에 본원 소아응급센터를 방문한 4,929명 중 621명이 입원했다. 이중 재방문 15명을 제외한 총 606명을 분석했고, 소아응급의학과, 소아과, 기타 진료과에 입원한 환자는 각각 91명, 456명, 59명이었다( Fig. 1). 세 군 사이에서 유의한 차이를 보인 변수는 나이, KTAS 1-3단계, 응급실 체류시간, 입원 후 결과, 입원 기간, 체온이었다( Table 1). 소아응급의학과 또는 소아과에 입원한 환자 나이의 중앙값은 각각 2세 및 1세인 반면, 기타 진료과 환자는 9세였다. KTAS 1-3단계 환자의 79.4% (400/504명)가 소아과에 입원했다. 진료과별로, 소아응급의학과(78.0%) 및 소아과(87.7%)가 기타 진료과(55.9%)보다 중증이 흔했다. 응급실 체류시간의 중앙값은 4.2시간이고, 소아응급의학과 및 소아과는 각각 4.3시간 및 4.0시간, 기타 진료과는 6.3시간이었다. 입원 중 전과는 소아응급의학과 및 소아과에서만, 중환자실 이송은 기타 진료과에서만 각각 확인됐다. 입원 기간의 중앙값은 50.0시간이고, 소아응급의학과, 소아과, 기타 진료과로 갈수록 길어졌다. 체온은 소아과에서 37.6 。C로 가장 높았다. 재방문은 소아응급의학과 및 소아과에서만 나타났고, 세 군 간 유의한 차이는 없었다.
2. 세 군과 응급실 체류시간 및 입원 기간의 선형 연관
응급실 체류시간의 중앙값은 소아과 및 소아응급의학과 사이에서 유의한 차이가 없지만, 기타 진료과 환자는 소아응급의학과 환자보다 1.538배 증가했다( Table 2). 입원 기간의 중앙값은 소아과가 소아응급의학과 환자보다 2.535배 증가했고, 기타 진료과 환자는 소아응급의학과 환자보다 3.375배 증가했다.
3. 주증상 및 주진단
상위 5가지 주증상은 빈도 순으로 열, 구토, 복통, 기침, 발작이었다( Fig. 2A). 열 환자는 주로 소아과에, 구토 환자는 소아응급의학과 및 소아과에 같은 비율로, 복통 환자는 주로 기타 진료과에 각각 입원했다. 기침 또는 발작 환자는 모두 소아과에 입원했다. 상위 5가지 주진단은 빈도 순으로 패혈증, 위장염, 요로감염, 충수염, 발작이었다( Fig. 2B). 패혈증, 요로감염, 발작 환자는 모두 소아과에 입원했고, 위장염 환자는 소아응급의학과 및 소아과에 비슷한 비율에 입원했다. 충수염 환자는 전원 기타 진료과(외과)에 입원했다. Appendix 1 ( https://doi.org/10.22470/pemj.2023.00794)에 주증상 및 주진단의 빈도를 진료과별로 나열했다.
고 찰
본 연구를 통해 다음 사실을 확인할 수 있다. 소아응급의학과에 입원한 환자는 비교적 높은 중증 비율(78.0%) 및 어린 나이(중앙값 2세)에도 불구하고 응급실 체류시간(4.3시간) 및 입원 기간(19.0시간)이 짧고, 재방문 빈도는 다른 진료과와 비교하여 차이가 없었다( Table 1). 소아응급의학과 환자의 응급실 체류시간 및 입원 기간이 짧은 경향은 기타 진료과와 비교할 때 가장 현저했다( Table 2). 소아응급의학과에서 가장 흔한 주증상 및 주진단은 각각 구토 및 위장염이었으며, 단기 수액요법을 위한 입원이 가장 많았다. 관련된 미국 연구는 소아∙청소년 환자를 대상으로 단기 치료 공간인 관찰 병동(observation units, OU)의 유용성을 보여준다( 14- 17). 그 중 외래 환자에 기반을 두고 기존 입원 병동 대신 단기체류병동(short stay unit)을 1년간 운영한 결과, 58%는 24시간 이내에 퇴원했고, 총 2,480일의 병원 입원 일수를 절약했다( 15). 최초의 소아 OU는 1970년경 입원 환자 수 및 기간을 줄이는 것을 목표로 시작했다. 이후 OU는 대개 24시간 미만의 치료를 제공하면서 기존 입원에 대한 안전한 대안으로 발전했다. 구체적으로 OU는 기존 입원보다 체류시간이 짧고, 입원율이 낮으며, 0.01%-5%의 재방문율을 보였는데, 7개 연구에서 기존 입원과 비교하여 OU 운영이 재정적 이점이 있다고 보고했다( 15- 17). OU에 입원하는 환자에서 빈번한 진단은 천식, 세기관지염, 크루프 등 호흡기질환, 탈수 및 복통을 동반하는 위장염, 두부손상, 약물중독 등이다( 18- 20). 본 연구에서도 소아응급의학과의 5대 주진단이 위장염, 뇌진탕, 실신, 중독, 상기도감염이라는 점은 이 환자군에서 경증이라도 단기 치료 또는 관찰이 유용하다는 점을 시사한다. 본 연구에서 소아과 환자 중 감염, 신경계, 호흡계 관련 주증상 및 주진단이 흔했다( Appendix 1). 소아과 환자는 단기 관찰보다 항생제, 산소, 기관지확장제 요법, 신경계 검사 및 관찰 등을 위해 입원하는 경우가 흔하다. 이와 대조적으로, 소아응급의학과에는 경증이지만 응급실 체류가 길어지거나 재방문 가능성이 높은 환자, 위장염으로 수액 요법이 필요한 환자, 두부외상 및 중독에 대한 관찰, 중증으로 진행하지 않은 상기도감염 환자가 입원했다. 즉 두 진료과의 입원 목적이 서로 다른 것이 주증상 및 주진단의 차이를 초래한 것으로 생각한다. 한국에서 응급의학과가 운영하는 성인 대상 단기 응급병동의 효과에 관한 연구가 있다. Ok 등( 21)에 의하면 응급병동 운영은 응급실 체류를 줄이고, 중환자실 입원은 응급병동 군에서 대조군보다 유의하게 드물었다. Moon 등( 22)의 연구에서는 응급의학과가 운영하는 응급병동에 입원하면, 일반병동 입원 또는 다른 진료과에 의한 응급병동 입원과 비교하여 평균 응급실 체류시간(7.1시간 대 8.0-10.2시간; P < 0.001)이 짧고, 원내 사망률(1.9% 대 2.2%-4.1%; P < 0.001)도 낮았다. 즉 응급의학과가 응급병동을 운영하면, 응급실 과밀화를 완화하고 예후에 긍정적 영향을 미칠 수 있다. 소아에서도 응급병동 운영의 효과를 기대할 수 있다. 실제로, 본 연구에서 소아응급의학과와 기타 진료과 사이의 응급실 체류시간 차이가 현저했다(4.3 대 6.4시간). 기타 진료과에 입원한 59명의 경우 외과 39명, 산부인과 7명, 신경외과 5명, 정신건강의학과 4명, 이비인후과 1명, 흉부외과 2명, 비뇨의학과 1명이었다. 대개 검사 후 수술이 필요하다고 확인되면 해당 진료과에 협진을 의뢰했고 이후 수술 준비 또는 입원이 이뤄져, 체류가 길어지는 경향이 있었다. 소아응급의학과와 소아과 사이에서 체류시간의 차이는 비교적 작았다. 이는 소아응급의학과 의사가 두 진료과의 입원을 모두 결정하는 본원 정책에 따라 입원이 빨리 결정된 영향으로 보인다.
소아응급의학과에서 전과된 환자는 4명(4.4%), 재방문한 환자는 3명(3.3%)이었다. 전과는 모두 소아응급의학과에서 소아과로 이뤄졌다. 이는 소아응급의학과 환자의 증상이 지속하여 입원이 길어지면서 소아과로 전과한 것이다. 구체적으로, 두부외상 관찰 중 두통 지속, 위장염 증상 지속, 상기도감염이 폐렴으로 진행, acetaminophen 중독 급성기 치료 후 장기 입원이 필요한 환자가 각 1명이었다. 재방문한 3명 중 같은 증상이 악화하여 재방문한 환자 1명은 구토로 입원 후 수액요법을 받고 퇴원했다가 2일 후 구토가 재발하여 재입원했다. 그 외에 보호자가 강력히 원하여 재입원한 환자와 퇴원 후 충수염이 진단되어 외과에 입원한 환자가 각 1명이었다.
2004년 Rentz 등( 23)의 보고에 의하면, 응급의학과가 운영하는 OU는 지역사회 및 전문 분야 의사로부터 모든 영역에서 높은 만족도를 기록했다. 60% 이상의 임상의사는 OU가 탈수, 위장염, 민감한 기도질환, 세기관지염 치료에 유용하다고 응답했다. 본 저자는 응급병동 운영 후 환자 및 의사의 만족도를 분석할 예정이다. 본 연구의 제한점은 다음과 같다. 첫째, 적은 수의 연구 대상자 및 짧은 연구기간으로 인해, 계절 요인을 분석하지 못했다. 둘째, 단일기관 연구라는 점이다. 보편적으로 적용할 수 있는 결과를 위해서는 다양한 기관과 공동으로 연구해야 한다. 셋째, 응급실 체류 지연의 복합적 원인 중 일부가 교란변수로 작용할 수 있지만, 이를 모두 통제하지 못했다.
소아응급의학과에 경증으로 단기 치료 또는 관찰이 필요한 환자를 입원시킴으로써, 응급실 진료의 질 향상에 도움이 될 것으로 생각한다. 응급병동 입원을 통해 체류시간을 줄이고 과밀화 해소에 기여하며 같은 증상으로 인한 재방문을 예방할 수 있기 때문이다.
Fig. 1.
Flowchart for selection of the study population. PEM: pediatric emergency medicine, PED: pediatrics. 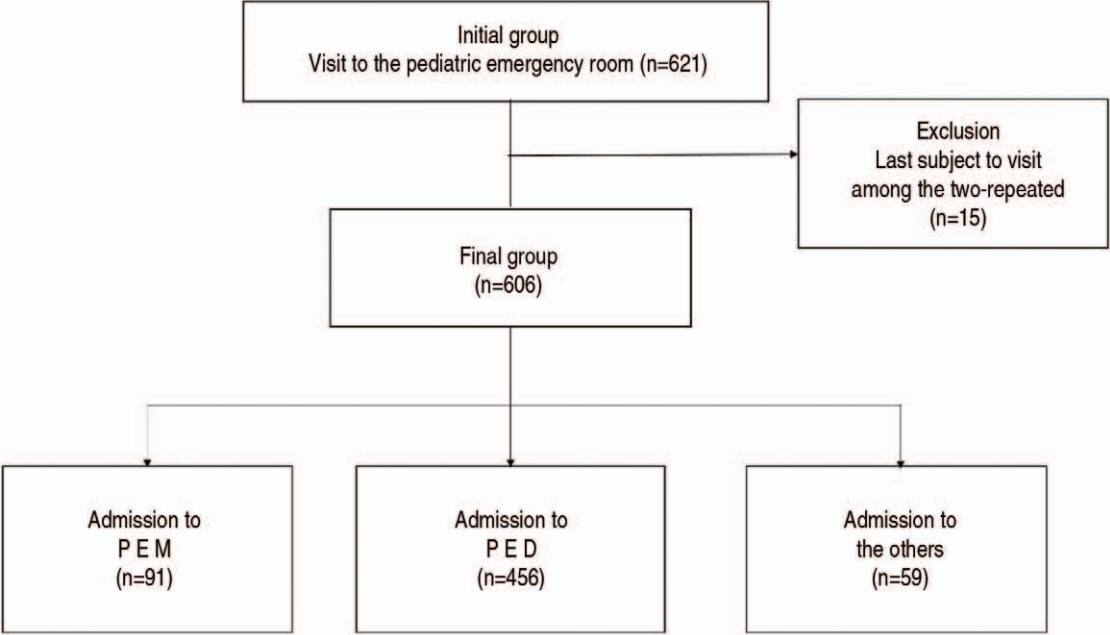
Fig. 2.
Top 5 chief complaints (A) and primary diagnoses (B). PEM: pediatric emergency medicine, PED: pediatrics. 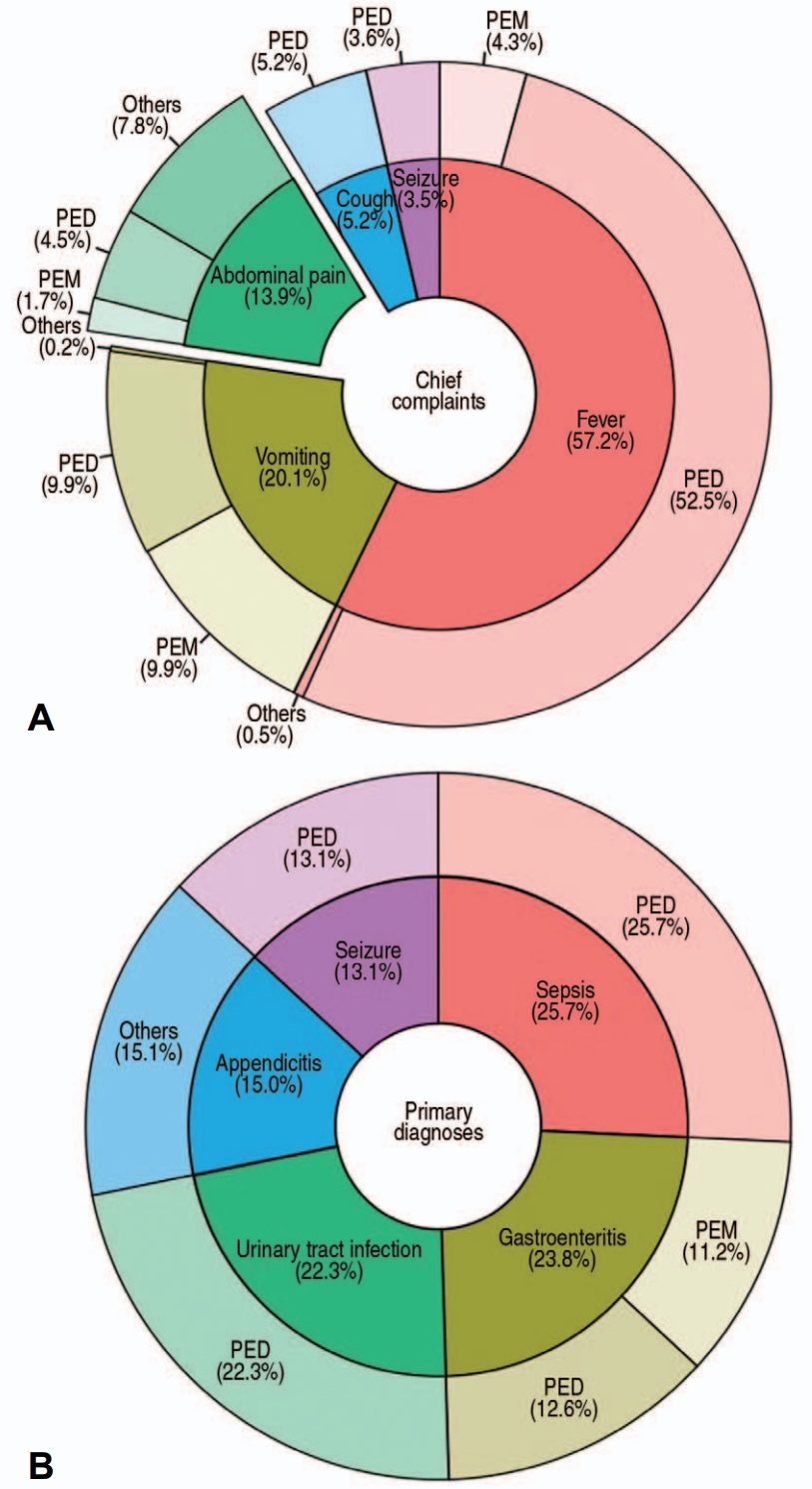
Table 1.
Statistical comparison for characteristics of patients according to PEM, PED, and others
|
Total (N = 606) |
PEM (N = 91) |
PED (N = 456) |
Others* (N = 59) |
P value |
|
Age, y |
1 (0-6) |
2 (1-60) |
1 (0-4) |
9 (7-14) |
< 0.001†
|
|
Girls |
290 (47.9) |
52 (57.1) |
209 (45.8) |
29 (49.2) |
0.140‡
|
|
KTAS 1-3 |
504 (83.2) |
71 (78.0) |
400 (87.7) |
33 (55.9) |
< 0.001‡
|
|
Ambulance |
66 (10.9) |
7 (7.7) |
55 (12.1) |
4 (6.8) |
0.268‡
|
|
Symptom-to-arrival, min |
791 (175-2,071) |
485 (134-1,425) |
850 (180-2,287) |
973 (288-1,851) |
0.111†
|
|
EDLOS, h |
4.2 (3.2-5.4) |
4.3 (3.1-5.2) |
4.0 (3.2-5.1) |
6.3 (4.8-8.2) |
< 0.001†
|
|
Disposition |
|
|
|
|
< 0.001§
|
|
Transfer to other departments |
22 (3.6) |
4 (4.4) |
18 (3.9) |
0 (0) |
|
|
Intensive care unit |
16 (2.6) |
0 (0) |
0 (0) |
16 (27.1) |
|
|
Hospital LOS, h |
50.0 (33.3-71.4) |
19.0 (13.9-32.7) |
58.5 (38.9-77.3) |
63.8 (43.6-98.4) |
< 0.001†
|
|
Temp, 。C |
37.3 (36.8-38.2) |
37.0 (36.7-37.5) |
37.6 (36.9-38.4) |
37.0 (36.6-37.2) |
< 0.001†
|
|
SPO2, % |
100 (99-100) |
100 (99-100) |
100 (99-100) |
100 (99-100) |
0.050†
|
|
Return visit |
20 (3.3) |
3 (3.3) |
17 (3.7) |
0 (0) |
0.394§
|
Table 2.
Simple linear regression analysis of factors associated with hospitalization to PEM
|
Department |
EDLOS
|
Hospital LOS
|
|
Estimate*
|
P value |
Estimate*
|
P value |
|
PED vs. PEM |
0.996 (0.911-1.088) |
0.922 |
2.535 (2.197-2.925) |
< 0.001 |
|
Others vs. PEM |
1.538 (1.353-1.749) |
< 0.001 |
3.375 (2.741-4.157) |
< 0.001 |
|
Overall significance†
|
NA |
< 0.001 |
NA |
< 0.001 |
References
1. Ministry of the Interior and Safety. Population statistics of Korea [Internet]. Ministry of the Interior and Safety; 2008-2023 [cited 2023 Mar 31]. Available from: https://jumin.mois.go.kr. Korean. 2. Noh H. Prehospital transport of critically ill children via 119 emergency medical service providers: problems and improvement plan. Pediatr Emerg Med J 2017;4:34–7. Korean.   3. Kim HM, Ha SO, Yang WS, Park YS, Kim JH. Effect of coronavirus disease 2019 pandemic on children’s visits to the emergency department. Pediatr Emerg Med J 2022;9:10–6. 4. Song WM, Noh H, Ahn KO, Jeong SY, Suh J. Utilization of pediatric emergency medical center depending on visiting time. J Korean Soc Emerg Med 2016;27:182–8. Korean.
6. Kim EY. Policy direction for the development of pediatric emergency care in Korea. Pediatr Emerg Med J 2023;10:1–2. Korean. 7. Noh H, Kim DK, Lee JH, Kwak YH, Jung JH, Jang HY, et al. Comparisons of pediatric patients who visited to the pediatric emergency department and the general emergency department. Pediatr Emerg Med J 2015;2:29–34. Korean. 8. Harper A, Jones P, Wimsett J, Stewart J, Le Fevre J, Wells S, et al. The effect of the shorter stays in emergency departments health target on the quality of ED discharge summaries. Emerg Med J 2016;33:860–4.  10. Shin S, Choi H, Choi B. Utilization characteristics of an advanced pediatric emergency center: a single center study over 2 years. Pediatr Emerg Med J 2020;7:16–22. Korean. 11. Kim JY, Choi SH, Yoon YH, Cho YD, Park S. Characteristics of recurrent visit of emergency department by pediatric patients. Pediatr Emerg Med J 2014;1:24–8. Korean. 12. Chai HS, Park GJ, Kim YM, Kim SC, Lee JH, Kim H, et al. Characteristics of frequent pediatric emergency department users at a tertiary university hospital. J Korean Soc Emerg Med 2022;33:421–8. Korean.
15. Gururaj VJ, Allen JE, Russo RM. Short stay in an outpatient department. An alternative to hospitalization. Am J Dis Child 1972;123:128–32. 21. Ok M, Choi A, Kim MJ, Roh YH, Park I, Chung SP, et al. Emergency short-stay wards and boarding time in emergency departments: a propensity-score matching study. Am J Emerg Med 2020;38:2495–9. 23. Rentz AC, Kadish HA, Nelson DS. Physician satisfaction with a pediatric observation unit administered by pediatric emergency medicine physicians. Pediatr Emerg Care 2004;20:430–2.
Appendices
Appendix 1
Top 5 chief complaints and primary diagnoses
|
No. |
PEM (N = 91) |
PED (N = 456) |
Others (N = 59) |
|
Chief complaint |
Primary diagnosis |
Chief complaint |
Primary diagnosis |
Chief complaint |
Primary diagnosis |
|
1 |
Vomiting, 42 (46.2) |
AGE, 51 (56.0) |
Fever, 222 (48.7) |
Sepsis, 127 (27.9) |
AP, 33 (55.9) |
Appendicitis, 31 (52.5) |
|
2 |
Fever, 18 (19.8) |
Concussion, 4 (4.4) |
Vomiting, 42 (9.2) |
UTI, 46 (10.1) |
Fever, 2 (3.4) |
Teratoma, 2 (3.4) |
|
3 |
AP, 7 (7.7) |
Syncope, 3 (3.3) |
Cough, 22 (4.8) |
Seizure, 27 (5.9) |
Suicide attempt, 2 (3.4) |
EDH, 2 (3.4) |
|
4 |
Head injury, 5 (5.5) |
Poisoning, 2 (2.2) |
AP, 19 (4.2) |
AGE, 26 (5.7) |
Anxiety, 1 (1.7) |
Pneumothorax, 2 (3.4) |
|
5 |
Poisoning, 2 (2.2) |
URI, 1 (1.1) |
Seizure, 15 (3.3) |
Pneumonia, 13 (2.9) |
Chest pain, 1 (1.7) |
Psychosis, 1 (1.7) |
|
|