







Introduction
Epiploic appendagitis is a rare cause of acute abdominal pain in children 1,2). This entity is caused by torsion or thrombosis of the arterioles feeding the epiploic appendages, 0.5-5 cm-sized adipose tissues located on the anti-mesenteric surface of the colon, and consequent ischemia 2-4). It mostly affects patients in their fourth to fifth decades of life, with a male predominance 4,5). It tends to be more common in obese population probably due to the presence of excessive adipose tissue and the larger epiploic appendages 5,6). It is difficult to diagnose epiploic appendagitis or exclude surgical emergencies, solely by clinical findings. Thus, imaging study may be necessary in emergency departments (EDs) 2,7).
Herein, we report a case of epiploic appendagitis of a Korean adolescent boy who presented with pain in the left lower quadrant (LLQ) lasting more than 10 days. This study was approved by the institutional review board of Hanyang University Guri Hospital (IRB no. 2022-06-004). This case highlights the need for imaging study for early diagnosis of epiploic appendagitis or surgical emergencies in children who visit EDs with pain in the LLQ without specific clinical findings
Case
A previously healthy 14-year-old boy visited the ED in April 2022 with pain in the LLQ lasting more than 10 days. The pain had aching character, occurred intermittently many times a day, and lasted for several hours once aggravated without identified aggravating factors, such as eating. He did not report nausea, vomiting or diarrhea.
The initial vital signs were as follows: blood pressure, 120/60 mmHg; heart rate, 80 beats/minute; respiratory rate, 20 breaths/minute; temperature, 36.5гҖӮC; and oxyhemoglobin saturation, 100%. He was 172 cm tall (75th percentile) and weighed 87 kg (> 97th percentile), making a body mass index of 29.4 kg/m2 (Z-score = 2.5). The initial physical examination showed unremarkable findings in the skin, head, ears, throat, chest, and extremities. Abdominal examination showed LLQ tenderness without abnormal bowel sounds and hepatosplenomegaly. There were no specific laboratory findings.
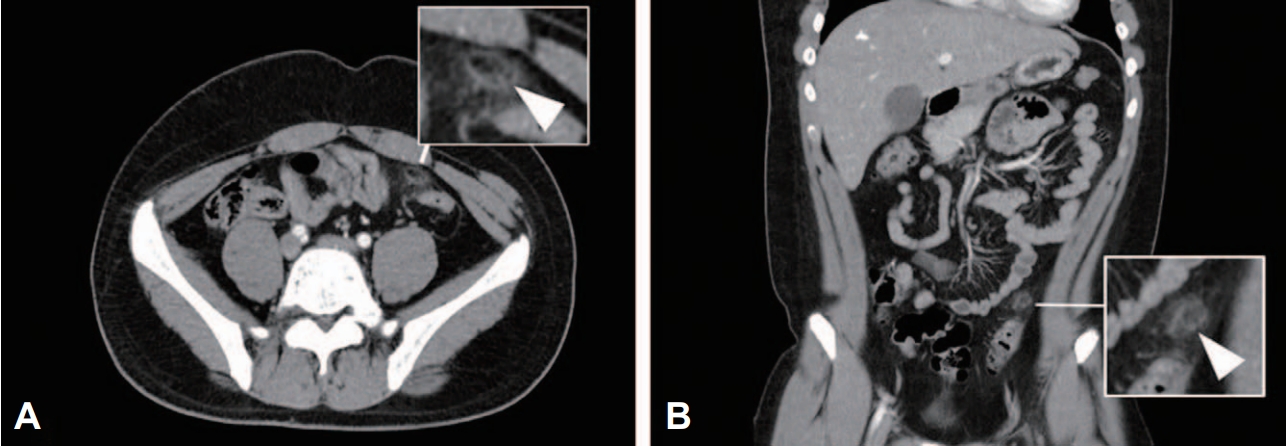
The initial plain radiograph showed the impacted feces (Fig. 1). First, glycerin enema was performed, followed by an observation period. Given the persistent pain, the boy was hospitalized to the ward. On day 2, computed tomography (CT) showed a prominent infiltration around the 1.8 cm-sized fat lobule in front of the sigmoid colon, leading to the diagnosis of epiploic appendagitis at the midsigmoid colon (Fig. 2). Although acetaminophen was administered for the initial pain control, the pain persisted. On day 6, a follow-up CT did not show improvement of the lesion.
The analgesic was then replaced by ketorolac tromethamine; subsequently, the pain gradually improved. On day 13, the pain subsided, and the boy was discharged. The conservative therapy was effective without a recurrence.
Discussion
In the present case report, we describe a 14-year-old boy diagnosed with epiploic appendagitis presenting with pain in the LLQ region persisting for over 10 days. Considered retrospectively, the case patientвҖҷs persistent pain in the quadrant, and obesity in terms of body mass index could have been the clues for diagnosis.
Diagnosis of acute abdominal pain in children is a common dilemma in emergency practice. Because many cases of the pain have a benign outcome, their pain tends to be underestimated in diagnosis, particularly in adolescents 8-10). However, in some cases, the clinical course can be improved through treatment based on rapid diagnosis. Thus, pediatricians or emergency physicians need to recognize the specific disease of which diagnosis can be supported by appropriate imaging study.
Localized abdominal pain without other symptoms is common in epiploic appendagitis. The pain related to the entity is cramping, typically focal, and self-limited within 1 week 1-3). Pain has been reported in the right lower quadrant and LLQ in 50%-55% and in 30% of patients with epiploic appendagitis, respectively 11,12). Therefore, if the pain persists, CT should be considered even if the pain is located in the LLQ rather than in the right lower quadrant, which has a high possibility of surgical emergencies.
Conservative therapy is indicated with analgesics. For this purpose, some studies suggest a need for oral anti-inflammatory medications 13,14). In the present case, the boyвҖҷs pain was relieved only after acetaminophen was replaced by a non-steroidal anti-inflammatory drug. The efficacy of specific analgesics is yet to be proven.